This post will give you the details you need to know about NSW Parliament’s latest inquiry into drug driving law reform and how you can lodge your submission. In doing so, you are expressing your unequivocal support of updated drug driving laws that include protection and defences for medicinal cannabis patients.
Lodging a submission can help restore freedom, support, and job security to the lives of thousands of medicinal cannabis patients in Australia.
What is a submission and why does it matter?
When the Government conducts an inquiry into an area of law–in this case, they’re revisiting the drug driving laws surrounding medicinal cannabis–the public has the opportunity to present a submission.
This submission is an opportunity to make your opinion known regarding the law in question.
Lodging a submission can be a powerful tool for advocacy in changing these laws. Government officials will consider these documents as they reformulate their thoughts or views on an issue.
Essentially, this submission is a tool to help you express your support of fair and equal drug driving laws.
What is the purpose of the Drive Change submission?
Written by ex-magistrate and director of Drive Change, David Heilpern, this submission expresses support for the Road Transport Amendment Bill.
In a nutshell, the Drive Change submission says:
All road safety data shows that there is not risk of increased road trauma from medicinal cannabis.
The current laws are discriminate against prescription medicinal cannabis users.
There is evidence to suggest those using other prescription drugs as an alternative to medicinal cannabis rose a greater risk to road safety.
The Tasmanian model and other international examples exemplify that the Bill’s proposed amendments are tried, tested, and safe.
The submission includes sources to scientific research and international law that supports the need for updated drug driving laws. Due 1 May 2022, the community has the chance now to essentially cast a vote and state the reasons for wanting change.
The Road Transport Amendment Bill would mean equal rights to medicinal cannabis patients who drive. That includes granting legal defence to patients who test positive in roadside tests for amounts of THC that are too low to cause impairment or are present in support of a prescription. The only state that currently grants this protection to medicinal cannabis patients in Tasmania.
Many medicinal cannabis patients are labourers who rely on their driver’s license to keep a job and support their families. The current laws discriminate against these patients and have the potential to upheave lives.
What if I don’t live in NSW?
You can still submit a submission if you do not live in NSW.
Getting the laws updated in the country’s most populous state would create an ideal model that other states and territories can emulate. Your own submission could become a catalyst for change country-wide.
A win for NSW is a win for all of Australia.
How do I lodge my submission?
1. Access the pre-written submission by copying and pasting from below or downloading the pdf from this link. You can also craft your own. Feel free to use ours as a template or guideline for your own.
2. Once you have the submission saved or downloaded, follow this link to access the submissions page for the “Road Transport Amendment (Medicinal Cannabis-Exemptions from Offenses) Bill 2021” on the Parliament of NSW website.
3. Log your submission:
Make sure the “Submissions” tab is selected. Then, click the button that says “to lodge a submission, click here.”
Select “submit as an individual,” and fill out your details.
Lodge your submission either by downloading the pre-prepared PDF or crafting your own submission. Feel free to use our document to help craft your own.
Finally, attach the downloaded file into the submissions page and submit.
All submissions for the Road Transport Amendment Bill are due 1 May 2022. Lodge yours now.
That’s it! Lodging these submissions allow you to speak directly to Parliament regarding the active conversation for updated drug driving laws. This is the perfect opportunity to voice your opinion and help make change happen.
As you may have seen, we’ve been encouraging the cannabis community to write letters to local members of Parliament. A major part of that campaign is to drive local MPs to the upcoming Drive Change Roundtable for Government officials.
What is the Roundtable?
This Roundtable will serve as a platform to address the discriminatory drug driving laws that are currently in place for medicinal cannabis patients. It is only open to MPs and Government Officials, giving them a chance to learn about and discuss the community’s call for change in a private forum.
The Roundtable will take place on Tuesday, 29 March 2022.
Leading up to this date, we are calling on community members to take a moment to tell their personal stories to MPs through letters. These letters are also an opportunity for the community to encourage MPs to attend the Roundtable.
By bringing your stories to their attention, they can bring your experience to the table. This is how change is made.
Why host a Roundtable?
It’s important that this cause is discussed amongst those who can make change happen. Letting your MPs know why drug driving law reform is important to you is a step towards enacting more fair and equal drug driving laws for cannabis patients.
As a patient or concerned citizen, how can I encourage MPs to go?
Write a letter to tell them your story, explain why reform is important to you, and provide details about the Roundtable. Attending this virtual, government-only event is their opportunity to show they are listening. Giving these officials a time and place to discuss it can be an effective means for getting law reform discussed in Parliament.
In addition to all government attendees, the Roundtable will also feature voices from healthcare, science, and law enforcement. These industry leaders all provide a valuable perspective on how the drug driving laws impact the community.
Teresa Towpik speaks from the perspective of a doctor, patient, and cancer survivor. When it comes to medicinal cannabis, she believes the laws are causing significant harm to people dealing with pain and illness in our society.
Dr Thomas Arkell Cannabis and Driving Research Expert working within the was previously a research candidate at the University of Sydney, where he earned his doctorate. Now he is a Research Fellow at Swinburne University.
Mick Palmer is a former commissioner of the Australian Federal Police. Reflecting on his career, he sees the driving laws as unfit-for-purpose and ends up punishing people already coping with a terminal illness or serious pain.
David Heilpern is an ex-magistrate, lawyer, adjunct professor, and the Drive Change campaign lead. He spent 21 years in Parliament, having been the youngest ever elected member, but left when he found there was too much restraint when it came to speaking out about drug driving law reform.
Fiona Patton (MP) is a leader of Victoria’s Reason Party. She is a vigorous voice in government for drug law reform and has submitted several proposals to the Victorian Parliament championing decriminalisation, cannabis for personal use, and drug driving law reform.
It’s time that Parliament hears the community’s support for drug driving law reform. Write your letter now and urge them to join the conversation with these industry leaders on 29 March.
Getting in touch with your local MP is one of the best ways to speak out in favour of the change you want to see in your community. Medicinal cannabis patients particularly have something that they should be speaking out about the discriminatory drug driving laws. We’ve organised a Letters to Local Members campaign to make it easy to get in touch with the representative for your area and be a voice for change.
Your letter to local members should share your personal experience with medicinal cannabis, how the discriminatory laws impact you, and why drug driving law reform is long overdue. By speaking directly to your local MP, you’re giving them a personalised reason to work toward drug driving law reform. We’ll give you everything you need to write a letter, identify your local MP, and send off your letter. All you need to do is tell your story.
The more patient stories and facts that representatives receive, the more likely they will become a voice for change in government. It all starts with telling your story. Your letter to a local member should be based on facts, but should also give them insight into the way the laws personally impact you. Get personal, speak from the heart, and give MPs a good reason to act in favour of drug driving law reform.
Your email or letter offers an opportunity to act immediately by signing up for the Drive Change Government Roundtable on Tuesday, 29 March. The Roundtable, open to government officials only, will provide a chance to gather for a discussion on the facts, science, and community call for drug driving law reform. Even if they can’t make be there, you should encourage them to sign up so they receive the recording.
A constituent voice–your voice–asking them to attend will make a difference.
The details of this event are provided in the letter for you.
What does this mean for you?
Your goal is to share your story. Easy as.
By writing your letter, you’re speaking out for the rights you deserve, and then giving MPs an opportunity to take action. Since the Government Roundtable will take place on 29 March, it’s the perfect chance for them to show up and prove they are doing something about the community’s needs.
Why should you write a letter to local members?
Your local MP is responsible for representing you in government and standing up for your rights. To do that, they need to know what you want.
By writing your story and citing scientific facts, you’re voicing a need for reform of the discriminatory drug driving laws. Sharing your experience can help catalyse change, so remember to let them know how the discriminatory laws are impacting you.
What it all comes down to is one simple fact: medicinal cannabis patients face discrimination. Speak out about your experience and then urge your local member to act on it by attending the Government Roundtable on 29 March.
What should the letter say?
This is your chance to get personal. Your letter needs to share your experience as a medicinal cannabis patient, and describe to your MP how the discriminatory laws impact your life, health, and livelihood.
The important thing to mention is how the discriminatory driving laws, and the restrictions on driving, negatively impact your life.
As an example, you may mention that your life-changing legal medicine is unreasonably at odds with the law. The only legal alternatives to medicinal cannabis are medicines like benzodiazepiness and opioids, etc. which are far more detrimental to your health and well-being.
Some other points to consider for your letter:
What is your medical diagnosis?
What was your health and well-being like before medicinal cannabis?
Why did you switch to medicinal cannabis?
How did cannabis change your life/health for the better?
How are the current discriminatory drug driving laws negatively impacting you?
Drug driving law: facts and figures
Medicinal cannabis patients face discrimination because the current laws don’t match the science. As you write your letter, it will be important to draw from the science to make solid arguments.
Browse the links below to gain an understanding of the studies and politics surrounding the drug-driving laws. You’ll find plenty of helpful stats and quotes within that will strengthen your letter.
Check back in this space regularly as we add more studies and resources.
Time to tell your story: here’s how
Once you review the science and are ready to tell your story, it’s time to write.
You can do this two ways:
To write an email, head to do-gooder to formulate your email and send it directly to your local MP. The templated paragraph included has details about the Roundtable ready to go along with your personalised story.
To write a physical letter, visit our Better Letters page, which is also set up with the information you need to spread the word about the upcoming event. When you select the tab “Write Your Letter”, choose the “Drive Change Template” from the dropdown menu under the Letters option.
If you don’t know who your local MP is, don’t worry. All you need to do is enter your address where prompted and it will send the email to your local rep.
Writing your letter to a local member is an integral part of taking steps toward change.
How else can I share my story?
Our plan for this campaign is to give the community a voice in the matter, and hopefully get the Government in favour of a change. The more ways we are able to reach out, the better. Sending a letter in the mail and as an email will make sure your story is heard.
Also, consider sharing your story with us! We are an authority for drug driving law reform and always welcome personal statements and patient stories. Email hello@drivechangemc.org.au with the title “Patient Story” and a photo of yourself (if you’d like) to let us know that you’d like to be featured.
Driving laws in Australia use a zero-tolerance policy for THC in drivers, despite the science that tells us THC presence has no bearing on intoxication. Wanting drug driving law reform is not a radical request. Several other countries have already amended their laws to allow medicinal cannabis patients to maintain their driving rights.
These countries serve as models for how Australia can adjust their laws to be less discriminatory. Take a look at some examples of updated protocols that can be used as a benchmark for drug driving law reform in Australia.
This information will be useful when you write to your local MP urging them to stand up for change!
California (USA)
The US State of California legalised medicinal cannabis in 1996. It was met with such success that the recreational mandate followed in 2016. Cannabis patients and purchasers have safely and successfully been on the roads since.
What many don’t know about this legalisation is that there is no legal bloodstream concentration limit for THC in the US state of California. Instead, California drug driving laws rely on field sobriety tests. These tests prove a more effective means for identifying drivers who pose a crash risk; THC metabolites alone are disproven as indicators of intoxication. Law enforcement is trained to detect impaired drivers and conduct these tests as needed.
A panel of experts led by the California Highway Patrol concluded that THC or THC metabolites in the bloodstream do not correlate with whether or not a driver is actually impaired.
Additionally, many Californian officers are specialists. There are 1700 specialists in the Californian police force that are certified Drug Recognition Evaluators. And California plans to train even more.
California’s Impaired Driving Task Force called to extend the required standardised field sobriety training from 8 to 24 hours, helping to improve detection of impaired drivers in roadside tests and help create safer roads.
These measures serve as a good example of how fair and just drug driving laws can be adopted as we move past methods that are proven to be outdated and inconsistent. California (population: 39 million) serves as a relatable example of how the laws will unfold in someplace like Australia (25 million people).
Canada legalised cannabis for adult use in 2018. Naturally, this raised concerns about the potential for increased traffic harm–a concern that Australia shares. But instead of maintaining outdated methods based on disproven science, the Canadian government mandated a periodic review of public health consequences of legalising cannabis. The most recent results were released as a report.
The report gathered records from all emergency departments in Ontario and Alberta–two states which account for 50% of the Canadian population. The data looked at moderate-to-severe traffic injuries that resulted in ER visits between April 1, 2015-December 31, 2019.
These inspiring results signal that, through effective laws and well-trained law enforcement, medicinal cannabis can be accessible to the adult population without putting a strain on safety in the community.
Police conduct routine traffic check in accordance with drug driving law.
Effective measures that end discriminatory laws
As we ask for drug driving law reform, we do so with real-world data and examples to show our legislature that it works to keep people safe.
Of course, even with laws in place, impaired driving remains a risk. This same risk is present with alcohol and other prescription drugs which are already given legal defence in roadsides. Doing so with cannabis is also possible, so long as law enforcement is properly trained.
1. Implement a Task Force
California’s Impaired Driving Task Force is dedicated to evaluating the factors at play for legal cannabis and adjusting the protocols to respond accordingly. Australia can create a similar team of experts to help adopt and enforce more effective policing measures.
For California, training law enforcement for signs of impaired driving has proven to be an effective measure for reducing incidents of impaired driving. With a task force in place, the state saves time and costly resources.
Australia still relies on breath tests for impairment. These tests are costly–a cost covered by taxpayers–and have a history of returning false results. California’s population is similar to that of Australia’s, so offers us a very realistic example of how such measures can be adopted here.
2. Train law enforcement in identifying intoxicated drivers
Another way Australia might be able to improve road safety by updating laws is to implement new training practices for law enforcement officials, as they did in Canada.
Canadian law enforcement is specifically trained to identify impaired drivers, helping to alleviate the need for faulty tests and mitigate road trauma. To conduct a roadside impairment test, Canadian Police may:
Administer a standard Standard Field Sobriety Testing (SFST). If the driver passes the SFST test, they are free to go. If they do not, they’ll be arrested to undergo additional testing.
Conduct a Drug Recognition Expert (DRE) evaluation, involving a series of tests and toxicology reports.
Require the driver to undertake an oral fluid drug screening
Demand a blood sample if there is reason to believe the driver committed an offence.
These Canadian practices offer us an example of cannabis policing that works to protect road safety and the rights of drivers who legally consume cannabis. Australia can do the same, but we’re not there yet. Our government still maintains outdated and costly practices that are proven ineffective and actively discriminate against legal patients.
Measuring impairment has more to do with the individual user, and much less with their blood content. While the drug driving laws continue to use blood and saliva as measures of impairment, up-to-date studies reveal the inaccuracy of these protocols.
One such study published in Neuroscience & Biobehavioral Reviews revealed that blood and saliva testing for THC has no actual correlation with impairment. Referencing their own studies as well as data from nearly 30 other publications, the research team was able to shed some light on the differences between measuring THC and alcohol in roadside tests, and which factors play a part in assessing impairment.
“Higher blood:THC concentrations were only weakly associated with increased impairment in occasional cannabis users while no significant relationship was detected in regular cannabis users.”
The science tells us that, when it comes to measuring cannabis impairment, several factors play a role. These include dose, mode of ingestion, and length of treatment.
A patient who has a long history with medicinal cannabis was less likely to register positive in roadside tests for THC, even when it is present.
Dose plays a large factor in the effects of medicinal cannabis, and low level prescriptions are still identifiable in roadside tests, even when a driver is unimpaired.
On the other hand, the research found that patients with a less frequent dosage would display a positive THC blood content in roadside tests. Police would interpret this as impaired, but do not take into account whether or not there are true signs of intoxication.
“This suggests that blood and oral fluid THC concentrations are relatively poor indicators of cannabis-THC-induced impairment,” says Dr Danielle McCartney
Despite these results showing that THC in blood has no relation to decreased driving performance, testing for presence remains the chosen mode of policing cannabis in Australia.
What can measure impairment?
How police will be able to accurately measure impairment and detect intoxication in drivers remains the biggest issue for medicinal cannabis patients and Australia’s road safety. However, the data provides a clear view into a method that is not working and opens the door to more effective opportunities.
“We clearly need more reliable ways of identifying cannabis impairment on the roads and the workplace. This is a particularly pressing problem for the rapidly increasing number of patients in Australia who are using legal medicinal cannabis yet are prohibited from driving.”
Professor Iain McGregor, Academic Director of the Lambert Initiative
One possible avenue that can help us better understand the effects of cannabis on driving is technology.
“Smartphone apps that may help people assess their impairment before driving are currently under development and may also prove useful,” said research and Drive Change ambassador Dr. Thomas Arkell
Ways to support Drive Change:
If the laws wrongly identify medicinal cannabis patients as intoxicated, while some drivers who are intoxicated do not register, then the laws are failing to effectively protect citizens on the road. It also discriminates against the thousands of medicinal cannabis patients who drive responsibly.
A word of caution: the science also tells us that drivers shouldn’t rely on their own judgment of impairment to deem themselves fit to drive. Instead, medicinal cannabis patients should be vocal about their condition, their positive experiences with medicinal cannabis, and how the discriminatory laws affect them. One way of doing so is by writing to local MPs.
We know that reaching out directly is one of the most effective ways to create change, and this is your chance to make it happen.
Last year, we saw our ambassador Cate Faehrmann call on officials to throw out all the roadside drug tests in Nimbin during Mardi Grass weekend, citing contamination. Now, she’s taking an even bigger swing at the unjust drug driving laws with the introduction of two new bills, and one of them may help us see our goal of more effective laws being realised.
The Road Transport Amendment Bill
The “Road Transport Amendment Bill” aims to give medicinal cannabis patients the same rights as any other patients in Australia who take prescription medicine. This means that they will not be penalised for driving if they have a valid prescription and can prove they are not impaired–the rights that all other patients also have.
Cate Faehrmann’s stance on drug laws in Australia align with the work of Drive Change.
A member of the Greens NSW, Cate Faehrmann is a vocal proponent of drug reform. She has introduced several bills throughout her career, but this one truly gets to the heart of the matter for medicinal cannabis patients and their rights to drive, something she says is “long overdue and increasingly urgent.”
This bill would amend our current driving laws, making them safer than they currently are and giving rights to medicinal cannabis patients. Drivers today are limited to medical options, like benzodiazepines, opiates, and morphine–which pose an even greater threat to road safety.
“I urge the Government and Opposition to assess my bill with compassion and common sense.”
Cate faehrmann, MP
“Roadside drug tests are incredibly sensitive. Patients can test positive 24 hours or more after they have consumed cannabis, well after any impairment has worn off.”
Cate Faehrmann uses scientific research to support the latest bills, and states: “This bill would simply provide the same medical defence that is already given to morphine patients. Medicinal cannabis is far safer than morphine on and off the road, but medicinal cannabis patients who test positive face damaging drug driving charges.”
If it passes, this bill will finally grant legal defence to medicinal cannabis patients who test positive in roadside tests, so long as they are within their legal rights and they are not impaired. Currently, the only state which grants this protection to medicinal cannabis patients in Tasmania.
Seeing this bill brought to the government means we may be able to see change soon, but it’s not guaranteed yet.
“It should have happened when medicinal cannabis was legalised at the federal level in 2016,” Cate Faehrmann says. “Instead medicinal cannabis patients have been discriminated against and forced not to drive because our laws haven’t kept up.”
What you can do to show support
As the government deliberates their stance on this bill, the community can urge them to enact the change we desperately need. Writing to your local MP is one way to ensure they know the community supports the implementation of these amended driving laws.
In conjunction with the Road Transport Amendment Bill, Ms Faehrmann also introduced the Cannabis Industry Bill 2021. This second bill aims to legalise medicinal cannabis for personal use. Though this would be an important step forward, protecting existing medicinal cannabis patients, many who have long been dealing with discrimination on the roadsides, is where we need to keep our focus.
Both of these bills will be up for debate in 2022.
With cannabis available via a prescription in Australia since 2016, both doctors and patients are increasingly more likely to consider it as part of a healthcare practice.
Medicinal cannabis is already widely prescribed for conditions including PTSD, chronic pain, anxiety, and insomnia. Although the health industry generally agrees with its medicinal merits, the driving laws still classify cannabis as a criminal substance.
Campaigns like Drive Change exist during this transition phase to help shape what drug driving laws will eventually look like.
Mat Henderson
This brings a lot of questions into view for patients who are prescribed medicinal cannabis, those who are interested in it, and the doctors who prescribe it. Some of the most persistent and important questions surround exactly how legal medicinal cannabis fits into the framework of current drug driving laws.
This was the focus of our first webinar, an Ask Me Anything-style event titled Ending Discrimination: Medicinal Cannabis & Drug Driving Questions Answered. With a panel of experts and a community of supporters, the conversation revealed a lot of confusion around medicinal cannabis’ legal standing on the roads.
These common questions give some insight into how the laws work currently, and how we plan to see them change.
Here’s a list of the questions in case you want to jump ahead:
Q: Why won’t politicians accept the science regarding THC and impairment, as they did for drink driving?
A: There are several reasons, most of which are residuals of the War on Drugs. Police are resistant to change roadside THC detection procedure. Even if they would consider it, there is currently no way to accurately measure someone’s impairment on THC as we can with alcohol.
There is also the pharmaceutical industry and lobbyists to consider. Big Pharma is king, and revisiting drug driving protocol would inherently mean putting benzo/opioids under the same microscope–something that no one wants to do for fear of ruffling feathers. Unless a corporation is willing to put the science of medicinal cannabis in front of legislators, it will likely remain under the radar. -Mat Henderson
Q: How developed are technologies to test for impairment? Are there any examples of such technologies used overseas? Are there better ways to test for impairment rather than RDTs?
A: Yes, we had an interesting session with the creator of
DRUID. Check it out.
Cannabis Patients Rights and Limitations
Q: Why can’t patients be given a medical card and/or use relevant TGA approvals to protect them at RDT?
A: It should be possible, but first we would need a change in the law. And that’s what we are striving for. –David Heilpern
Q: Are there documents or laws we can cite that will protect those of us that use this medicine responsibly?
A: Sadly, no. Mere presence without impairment is still presence and that’s all that matters under existing laws. – Mat Henderson
Q: Can TGA create a database of current patients for police, or would this be a breach of privacy and information?
A: It would be easy to set up with the patients permission, but can only happen if the law changes. -David Heilpern
Q: Do you think it’s possible that we will see a National approach to driving laws and driving law reform anytime soon?
A: Within the next ten years or not at all. – Mat Henderson
Q: Is there any legal standing for patients to deny a RDT?
A: Like Random Breath Testing (RBT) for alcohol, you can be charged as if you failed the RDT if you deny taking one. -David Heilpern
Q: Why does the law target THC when there are so many other legal or illegal substances which cause worse impairment?
A: Simply because of the historical hangover from the War on Drugs where THC was primarily associated with recreational cannabis. This association still exists. We are living through a transitional era where the law will eventually align with the new reality that THC is also a prescribed medication. Precisely what that regime eventually looks like is anyone’s guess, but campaigns like Drive Change exist during this transition phase to help shape what those laws will eventually look like. – Mat Henderson
Q: Is it fit and proper for police to be advocating for the law and to determine public policy on health outcomes?
A: There is no problem with the police union speaking out, or the police minister. That is their role and function. However, police are meant to apply the law, not comment on it. It is our opinion that these comments ought not be aired in public. What politician would have the guts to go against the police? The police know this, and use their power. It is wrong. -David Heilpern
Q: Why do the police have vested interests in keeping these current laws and how can we better educate them?
A: The police in NSW get a budget allocation directly from Road Safety to administer the tests, thus the police have a vested interest. -David Heilpern
How to Help Drive Change
Sign the petition, which helps us to prove to lawmakers how much support is in favour of drug driving law reform.
You can also help support the ongoing cause by donating to Drive Change.
This article is written by Drive Change ambassador Dr. Teresa Towpik. Below, she shares her experience with the drug driving laws from the standpoint of a medicinal cannabis doctor and patient.
January 2016–what a month it was for me.
I didn’t realise it then, but this would mark the beginning of a new chapter in my life. This was when I first heard that cannabis was going to be legalised for medicinal use.
At the time, I was extremely surprised. I didn’t even really understand cannabis. To me it was better known as marijuana, a drug of addiction; dangerous and to be avoided.
However, once I started to do my research, I realised how wrong and ignorant I had been.
It soon became clear to me that I was now dealing with an amazing herb that has incredible medicinal and healing properties. I felt touched and inspired by patients’ stories, especially children suffering from intractable epilepsy. I began to see cannabis as a sophisticated plant.
In learning all this, I discovered that I wasn’t able to be passive and conveniently wait for others to speak up about this. I decided to become an advocate of cannabis and committed to long hours learning about this plant.
Real-World Use
I made the decision to become involved in prescribing cannabis as a doctor. It was a difficult process to begin, because the access to cannabis was cumbersome and convoluted. It required hours of paperwork that turned into countless rejections from both TGA and NSW Health State Department.
I first applied to the TGA when I had a patient who suffered from Parkinson’s disease. The application to prescribe was approved by the TGA in September 2017, but NSW Health kept rejecting it. There was a lot of back and forth, even a solicitor was involved.
Finally, in March 2018, I got my approval. It seemed the floodgates were open, and after that every application was approved within 48 hours.
Since then, I have prescribed cannabis for many patients and have observed how it changed them for the better. Many of my patients became more functional, alert, and active. A few of them even said to me “my brain is not so foggy anymore.”
I have seen firsthand the positive effects cannabis has on these patients. For many of them, cannabis offers a return to normalcy, reinvigorating their functionality, motivation, and inspiration in life. It’s the key for them to return to working jobs, socialising, and living a full life.
Cannabis and Road Safety
Unfortunately, there is a very significant roadblock to improving patient outcomes through prescribing medicinal cannabis in Australia. That roadblock is the discriminatory and unfair drug driving laws on medicinal cannabis patients.
These laws are causing significant harm to many people dealing with pain and illness in our society. Many of these are people who have exhausted various therapeutic options in treating their condition with no success. Eventually, they come to think and feel that they are forgotten by the health system.
Medicinal cannabis makes it possible for patients to leave behind days of taking 10-20 different medications, many of which reportedly makes them feel like zombies.
Some patients said that there were instances where they wouldn’t even remember how they managed to get from point A to B when driving on conventional prescription medicine.
I have had many patients comment that they became better drivers while taking cannabis. As a doctor I had to ask myself: what do I do in this situation? Should these people be reported for breaking the law?
Doctor, Advocate, Cannabis Patient
Through my professional experience I can tell you that the current drug driving laws limit clinical decisions. For many practitioners, the choice is often based not on what patients need, but on what the driving laws allow. Unfortunately, the laws don’t quite make sense.
Roadside tests currently screen for THC in the system as defined by a mouth swab. Any amount present is considered a criminal act. However, there is clear scientific evidence which proves the level of THC in the system does not correspond with impairment. If it did, I might be classified as a criminal myself.
In 2001, I was diagnosed with metastatic breast cancer. In May 2019, we discovered it was recurrent.
To cope with the effects of my cancer treatment, I have been taking significant doses of cannabis for the past 2 years. When I am not impaired, I have been driving. It is extremely unfair to know that the system labels me a criminal in this situation.
I am aware of the law’s zero-tolerance for THC, even for medicinal cannabis patients, but the fact is that I need my car to function. This is a situation that many patients experience in their lives, and no one is exempt from roadside drug testing.
I was drug tested on my way to Nimbin on 2 May of this year. Aware that this was a risk, I skipped my cannabis medication for 2 days before my trip. Still, my heart sank when I was stopped by the police. A lot went through my head, all the possibilities and consequences of me possibly testing positive. The fact that I have to deal with living in fear of being penalised for dealing with my condition feels terrible.
We know that cannabis is fat soluble and can stay detectable in the system much longer. Luckily, I tested negative. For me the trace amounts of THC was gone in two days, but this time frame varies by person, in part due to the rate of metabolism. I was not impaired and my driving record remains in good standing, but many patients feel like they are constantly at risk of losing their license. Patients have also told me that they feel more alert on medicinal cannabis than other drugs, yet they still face penalisation for the former. Feeling more alert makes sense because cannabis is proven to have a lower crash risk than many other drugs.
As a doctor and cannabis patient I am now standing up to the government in favour of appeal of these unfair laws and this unfair situation. Until this happens, I’m left with the question: is it moral to obey immoral laws?
To help change these unjust laws, please sign the Drive Change petition.
Blake is sharing his experience as part of our “Personal Stories” series, which invites medicinal cannabis patients to share with the community how drug driving laws are impacting their quality of life. If you’d like to share your story, please email us at hello@drivechangemc.com.au
It’s time that medicinal cannabis patients in Queensland are given driving defence.
I’m a medicinal cannabis patient, and every day I worry that if I were to get drug tested that it would screen positive.
It’s not fair that I should have to worry about this, since using my medicine doesn’t mean I drive when I’m impaired. Having access to medicinal cannabis has been a godsend for my condition, but knowing about the consequences if I test positive in a drug test only brings anxiety.
I use medicinal cannabis to treat my bipolar disorder. I’ve grappled with this for a long time, and access to medicinal cannabis has helped to save my life.
However, the laws make it seem like the system still doesn’t accept medicinal cannabis. It’s unreasonable to suggest to people who use medicinal cannabis that they can “just go without for a few days” to be able to drive. The laws should take into account having THC in your system doesn’t mean you’re impaired.
I have the proper paperwork from the TGA, stating that THC may take up to five days for most of the THC to leave your system. To be able to work, I can’t wait that long before driving again. These laws are keeping me out of work and struggling to earn an income. If I choose to drive anyway, I am at risk of losing my license, even if I’m not impaired. It’s just not fair.
David Heilpern wrote a letter to the Land Transport Safety and Regulation department inquiring about the state of the current laws and in light of the research showing their ineffectiveness. The General Manager, Mr Andrew Mahon, answered this inquiry in a letter which we have attached below for reference.
The following is an open letter to Sussan Osmond, who Mr Andrew Mahon advised Drive Change to contact for further correspondence.
Dear Sussan Osmond,
I recently wrote to the Department of Transport and Main Roads expressing my concern over the ineffective and discriminatory drug laws in place for drivers. In this letter, I will address the Department of Transport and Main Roads directly.
What I presented to you was a concise report on how our drug driving laws are failing to improve safety as they discriminate against medicinal cannabis patients. While I appreciate your effort to offer a response, they were mostly evasive of the problem and prove that lawmakers aren’t relying on science or fact to formulate these laws. They are in need of an update.
In your response, you went as far as to agree they are “difficult to address” but failed to present any scientific evidence in support of the need to uphold the current jurisdiction. This proves a clear need for deeper understanding of the issue. I will provide that to you, and the wider community, here.
Cannabis as a drug
Cannabis is a drug that is proven to impair cognitive and motor function.
Mr. Andrew Mahon, Land Transport Safety and Regulation), QLD
In your letter, you address cannabis as a drug that is “proven to impair cognitive and motor function.” While this is true, it does not explain why the driving laws permit drivers to use other TGA-scheduled and over-the-counter drugs while operating vehicles.
This is the true crux of the issue between medicinal cannabis and roadside drug tests. The chemicals in pharmaceutical drugs can be detected with such tests. Conversely, cannabis can remain at detectable levels in these tests far beyond the time of impairment. This clearly points to current practices as the problem. Why are we still using outdated methods for roadside drug testing if we know without a shadow of a doubt that they’re unreliable?
That truth is that yes, cannabis is a drug. The wider truth of it is that there are plenty of drugs which get protection or a pass when they are detected in roadside tests. It is nothing short of discriminatory to deny such rights to medicinal cannabis patients, especially when you consider the effects on road toll.
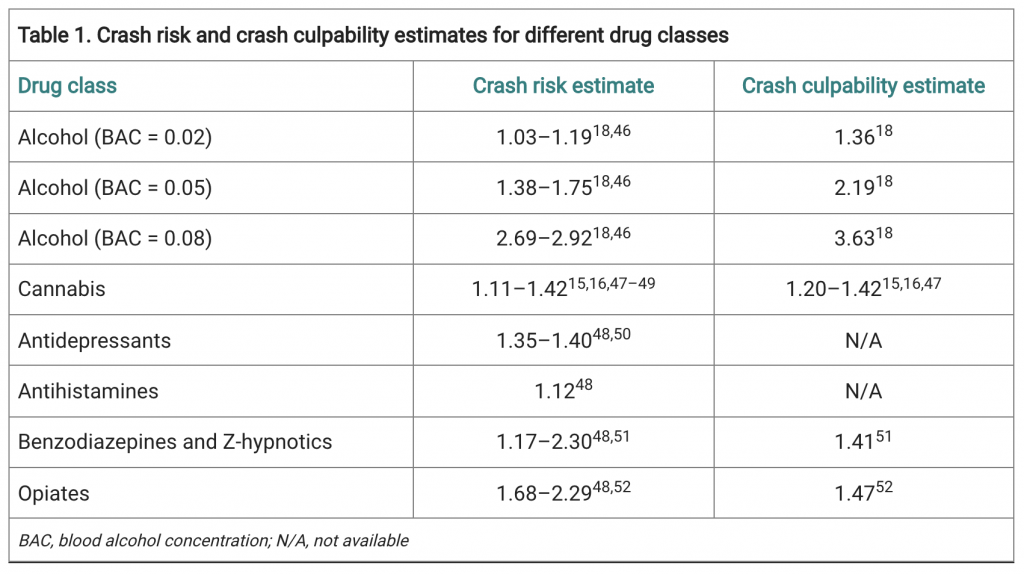
This has been an area that has been studied, and the results speak for themselves. The crash risk rate of drivers with a legal 0.05 BAC is 1.38-1.75. Once the BAC hits 0.08, this risk rises to 2.69. This is by far the highest crash risk rate of any of the other “impairing substances.”
Medical cannabis and driving, by Thomas R Arkell, Danielle McCartney, Iain S McGregor, doi: 10.31128/AJGP-02-21-5840
Opioids are not far behind, presenting a crash risk of 2.29; Benzodiazepines carry a risk up to 2.30. Even antihistamines carry a crash risk of 1.17. So why then, if cannabis carries a crash risk of 1.11-1.42, is it the only of these drugs to be banned on the roads?
Discrimination, again, seems to be the only plausible answer.
These discriminatory laws seem to be rooted in an outdated and unreasonable vilification of cannabis, one that doctors and scientists are committed to re-educating the public on. In some capacity, the government is already on board, having approved medicinal cannabis for therapeutic purposes, and there are 75,000 patients in Australia with legal prescriptions.
While these medical professionals have done their due diligence, there has been no accountability from the Department of Transport and Mains Roads, nor the police, in understanding that cannabis as a legal drug holds value in public health.
Driving and Road Safety
The role of drugs, in varying forms, is a growing problem for road safety, not only in Queensland but nationwide and internationally
Mr. Andrew Mahon, Land Transport Safety and Regulation), QLD
The TGA has categorised some forms of medicinal cannabis as a Schedule 8 Controlled Drug. Also in this class are Oxycontin, Sativex, Amytil, etc. So, why is it that patients who test positive for these conventional medications are not committing a crime while medicinal cannabis patients are?
In your letter, you mention that “The role of drugs, in varying forms, is a growing problem for road safety, not only in Queensland but nationwide and internationally.” I absolutely agree with you on this point, which is why I am so adamant about adjusting the laws surrounding them.
The studies into road safety measures speak for themselves in this matter. After the introduction of seatbelts, there was a marked decline in road deaths. Likewise with airbags. In terms of roadside testing for cannabis, there has been no evidence that this decreases road toll. This points to the fact that we need newer methods of understanding what leads to crash risk.
A “zero-tolerance approach” to selected legal prescriptions is clearly not the answer.
You mention that we “take a zero-tolerance approach through presence based legislation as opposed to setting limits similar to alcohol,” but this argument is also untrue and shows the lack of research that’s been done on this topic. Tasmania has adopted laws protecting medicinal cannabis patients on the road. It proves that it is being done here in Australia and can be done throughout the entire country to defend medicinal cannabis users without a toll on road safety.
Yes, impairment increases risk of motor vehicle crashes–which is exactly what roadside drug tests should be looking for. You seem to understand this, saying that “impairments that will affect a person’s driving include their ability to anticipate hazards and unexpected situations, their decision making and their ability to respond quickly to changes in the traffic environment (e.g. reaction time).”
I ask again – why can other potentially impairing pharmaceutical medicines get a pass in roadside tests? Additionally, in testing for the presence of THC, which remains detectable past the point of impairment, it seems that there is no real evidence to back your claim that this is in the name of road safety when other harmful drugs are permissible and protected.
The bottom line on mouth swabs is that they do not work. If they did, we would not have seen a 55% increase in road crashes between 2012-2018.
I do agree with you on one point, that medicinal cannabis cannot easily be tested at the roadside. The legislation stops short of the true issue: what can we do that can make road safety a priority, without a discriminatory framework that infringes on public health?
New and Improved Methods
The answer is not as elusive as you state it to be. In actuality, a simple impairment test can be completed. This has been successful in jurisdictions around the world. It has even caught up to the technological age, and apps such as DRUID app takes the guesswork out of it. Why is it that the Australian governments want to hold on to archaic methods of testing for drug impairment. It seems odd to want to do so when the equipment is so expensive and road toll even more costly both financially and from a human perspective.
I myself am acutely aware of these facts. But the truth of the matter is that the law is changing as our society begins to understand how to better care for our people. This is apparent when you consider the doctors, scientists, and lawyers who prescribe medicinal cannabis and/or support changing these discriminatory laws.. What is not apparent in your letter or in the law is why the Road Commission remains incredibly hesitant to take the step forward not only to assist in public health and putting an end to discrimination, but also into ways that have already proven capable of making our roads safer.
We are calling on your department and other governmental organisations and those in Parliament to research the facts. This is integral to the protection and progression of Australian medicine. This is about public safety and the knowledge of the facts to help improve public health and safety.
I trust this has given you some facts you may not otherwise have known.
The Drive Change team and more importantly patients who desperately need your assistance will await your response on this matter.
Yours sincerely,
David Heilpern
Director of Change
Drive Change
The original letter sent to Drive Change can be found here.
The letter above is a slightly edited copy (due to the different medium) of this letter.