“On Wednesday 19 March 2025, I secured the support of the NSW Legislative Council calling on NSW Police, NSW Health and other relevant government agencies to release all data relating to mobile drug testing and medicinal cannabis.
There is currently a distinct lack of available data and information to assess the value and effectiveness of the mobile drug testing program. I’ve asked for documents that detail the number of positive and false positive tests broken down by drug type, and the data on positive tests of THC for drivers who have a valid prescription for medicinal cannabis.
The motion also requests the cost to the taxpayer of conducting the mobile drug testing program and how the funding is provided to the NSW Police for the program including the annual budget, the cost of each initial test and any external contracts and consultants for the program.
This data will help us analyse exactly how many people are having their lives impacted by these unjust laws, and at what cost to the taxpayer. It will ensure the government is transparent about the effectiveness of this program, and guide our next steps in the campaign to legislate a fair defence for medicinal cannabis users on the road.
A massive thank you to everyone at Drive Change and the Cannabis Law Reform Alliance for leading the charge on roadside drug testing law reform.”
This report provides an overview of recent data provided to the Legislative Council by the Minister for Police and Counter-terrorism in New South Wales on 10 September 2024, with regards to roadside drug tests conducted over the last 5 years (by Local Area Command), number of positives by drug type and whether there has been improvements in road safety from the rollout of mobile drug testing programs (MDT) in NSW.
“While prescriptions for medicinal cannabis in Australia have continued to increase since being legalised in 2016, patients are unable to drive due to current drug driving laws and can be subjected to MDT programs which are conducted across New South Wales.
There is a distinct lack of available data and information to assess the value and effectiveness of the MDT Program. We urgently seek the NSW Government’s commitment to transparency of documents and data around MDT.”
Imagine having to choose between taking your legally prescribed medication and going to work,doing the school run or getting the shopping that week. Yes, week.
This is the stark reality for many Australian medicinal cannabis patients because of the discriminatory drug-driving laws that still exist in most states. Current laws penalise the mere presence of THC, not the driver’s impairment. The situation is compounded by the fact that THC can be detected through roadside drug tests for days after use. Consequently, many Australian medicinal cannabis patients find themselves having to skip their medication for multiple days before driving or risk legal repercussions.
To be clear, we wholly support measures to keep our roads safe, but penalising presence rather than impairment is patently unfair. No other legal prescription medications are treated in this manner.
Kindness, patient support and removing barriers to access are core parts of our brand, so for us, it’s a very simple matter of principle. We need to support our patients and advocate for their rights and wellbeing.
The path to reparation requires a two-pronged approach. First, we must advocate for legal reform that redefines the standards for determining a medicinal cannabis patient’s fitness to drive. Second, legal assistance should be provided to those patients who have been wrongly charged.
If our industry is to thrive, we must ensure that our patients enjoy the same rights and treatment as they would with any other legally prescribed medication. This is precisely why initiatives like #DriveChange are so important. I hope to see more of our industry peers rallying behind these crucial causes. Change is the only way forward.
If your prescribed medicine prevents you from driving and working, what does that mean for your human rights?
The UK’s Cannabis Industry Council released a report this week into workplace issues for medicinal cannabis patients who are regarded as disabled under UK work, health and safety laws. Despite its specificity, it is a worthwhile read for us in the Australian space.
When it comes to the British colonies of the Australian mainland and adjacent islands, Workplace laws ought be clarified to explain that when an employee asks for reasonable adjustments to be made on the basis of a temporary illness/permanent disability requiring them to take a medication outside of work hours that all medications ought be treated the same. As a Uno card, that’s a Draw Two right there. Problem being that employer medico-legal advisors flag unknown risks due to the current lack of an impairment proxy for THC. They need to cover their backsides and record that they advised their clients to exercise caution. The takeaway for many employers is “don’t hire the stoner, hire the other lady.” in work, health and safety terms, that’s a probable Draw Four.
Am sure that those who monitor the MC socials noted an uptick in hospo workers reporting pre-screener issues when a medicinal cannabis prescription is disclosed. These people are doing the right thing. As is usually the case when legal medicinal cannabis butts up against prohibitionist-era-oriented legal and social institutions, these people doing the right thing get punished for doing so.
How do we get this clarification that MC ought be treated the same as other prescription medicines? A few ways. With a series of sensible workarounds likely to be discussed in the upcoming Victorian LCA’s review/committee/process to have an adult discussion about fixing this so that the hospitality industry (at-least) doesn’t come to a screeching halt.
Another way is for clarification to be expedited by way of a matter/case with good facts and NO whiff of non-medicinal cannabis use going through various courts and tribunals. That will certainly provide guidance.
For readers who know him, it won’t come as a surprise that Veteran advocate Derek Pyrah is already aiming up at a Human Rights angle for all veterans to received subsidised MC, even on MH-only grounds. An opinion via a senior HR counsel is in the works but it will take some time. Derek’s arguments are also applicable to the MC and workplace and driving issues.
Ultimately it’s a question of whether Adequate Medical Care in Article 25 of UN Declaration of Human Rights means whatever The Literature says or whether there is scope for a human rights angle in circumstances where a person can demonstrate that harms were caused by an unwise and voluminous combination of prescription drugs over many years?
The DSM says that Derek received nine years of the best mental health care that any system could offer. Five of them separated from Missy as a result of being on psych wards. Everything from antidepressants, antipsychotics, sleeping pills and opioids. But all at once and in large amounts. You try lifting your head on 1800mg of quetiapine.
Is there a court on earth that would believe Derek’s subjective opinion on whether CBD:THC is more safe and effective for him than whatever the prevailing wisdom of the prestigious Medical Colleges and prevailing expert psychopharmacologists say? Would any of those academics accurately be able to tell you which picture of Derek below is the guy who vapes (but used to smoke) cannabis and which is the guy taking his many different prescription medicines as directed?
For workers faced with the conundrum of going back to the meds that didn’t work and/or harmed them, the immediate gut feel of adverse action being taken them is that their human rights are being violated. In some Australian jurisdictions this is worth a closer look when it comes to the nature of their work and the actions taken against them.
If a worker being prescribed THC oils or flos for nighttime/bedtime/non-work days only for:
Specific indications “ABC/XYZ”; and
As a harm reduction measure from many years of using tobacco spin and combustion + lowering overall THC consumption.
If you’re a doctor scratching your head wondering how you’re going to frame a letter to an employer for this class of patients then please get in touch.
Drive Change’s David Heilpern got some great soundbites in last Saturday morning and ABC News ran them on the hour, every hour, all day. This is the benefit of having elected reps in Victoria, WA and NSW bringing on topical parliamentary debates on cannabis law reform. Journalists will ring us to discuss this News, interview us and then items are broadcast as News because debates on the floor of parliament are News.
Now for for another novel workplace situation from this past week. Doug (not his real name and three situations merged into one here) was always shy and withdrawn. Spends a lot of time online. Occasional bouts of sadness due to isolation and feeling out of place in the world. Conventional cookie cutter mental health services and the DSM had the guy on the SSRI-benzo conga line from the age of 16-36. Doug didn’t have many good days in that time.
After 18 months on CBD daily and THC at bedtime (and tapering down to half dose of an SNRI). Doug has started reporting this new thing. Good days.
Doug’s job is to sit behind a computer and purchase things by mouse-click and do his bit in a supply chain. Good worker. It’s a good job, good crew. Everyone’s matey. Outside of his online world, these work friendships are key keeping Doug socialised.
People noted he was a different (better) guy the last 18 months and commented on him coming out of his shell and smiling a bit more. Poor Doug fell victim to the human tendency of confiding in the people we share our workdays with.
Noelene from Accounts: Did you hear?
Nelly from Marketing:About Doug, yeah. Good on him. He seems to be doing better and he’s happier. His work certainly hasn’t suffered.
Noelene: No, because it’s the medical cannabis with THC in it they stood him down pending a big chat between doctors and lawyers.
Sure enough, HR bundled him off home and had their own expert medical advisors look into this medical cannabis stuff. Doug got good letters and support from his MC prescriber. Doug didn’t have a list of high THC flos prescriptions longer than a Leonard Cohen song (to quote the fictional Malcolm Tucker). Doug has a CBD isolate oil by day, a dedicated night time flower with a vanilla and not-rasta-sounding product name for bedtime. Strain/Chemovar names are what they are. They are the inchoate property marker hangover from the prohibition era when breeders of cannabis phenotypes couldn’t exactly defend rights in their creations in the courts but those creations needed names and many of those names are derived from the unique terpene bouquet given off by that chemovar.
Some employer-side advisors grasp this and can gloss over the product being prescribed having [insert whacky strain name] and focus more on:
What are the conditions being treated?
What is the ratio of cannabinoids + dose being used to achieve a therapeutic benefit? What times of day/night are doses taken?
Is there reasonable basis to claim that all conventional meds have failed to achieve the same benefit and overall improvement in quality of life?
Guess what? Common sense prevailed. Doug will be welcomed back to full duties after a 4 week stand down.
But there are other ways employers can move people on and MC patients will always feel extra vulnerable in uncertain economic times. This means the R word (redundancies) but it can also mean adverse action via means that are hard to challenge, esp for gig economy delivery workers who need their licenses.
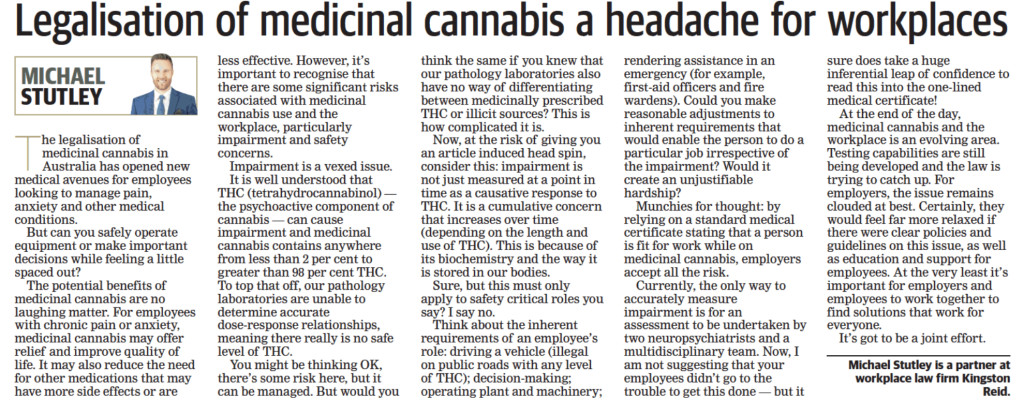
The below article penned by Perth-based workplace lawyers appeared in the West Australian on 18 August 2023. It catastrophises the brave new world of Medicinal Cannabis permeating our everyday lives, including our working lives.
It is an interesting piece but also a bizdev exercise that deserves a swift rebuttal from Drive Change alongside some general commentary on a couple of points where we somewhat agree.
One line medical certificates doled out by telehealth-only operators are not useful in broadening corporate and industrial acceptance of cannabinoid therapeutics. CBD and THC are viable treatment options for people where past use of SSRIs, benzodiazepines, opioids, gabapentinoids and quetiapine (to name but a few other types of impairing drugs) has not alleviated the symptoms being treated or caused intolerable side effects.
Online-only operators need to go that extra step in dealing with employers. Not ditching patients caught in a bind would be useful also. Providing patients with something more than one line or tangental boilerplate on why you can’t provide a more detailed letter without physical examination. Failing to offer something beyond the bare minimum for telehealth patients caught up in workplace drug testing issues is, being blunt, a dick move.
In a post-Covid industrial world where battle lines are now being drawn over WFH (work from home), employers also need to get to grips with the fact that many workers utilised the lockdown era as a chance to finally taper off the many prescription drugs that were harming not helping them. Mainly SSRIs if you place any stock in the wonderful world of Reddit and closed social media groups for persons tapering off X drug.
The lockdown era assisted many in dialling back on poly-pharmacy generally. The chronic-insomniac-in-lockdown had leeway for some intentionally rough nights withdrawing from benzos because they knew that holding it together in a Zoom meeting the following day was doable. But fronting up to the office in person, forget it. The warehouse worker who was reliant on opioids to get through each shift was able to dial back their dose of oxycontin to half (and gradually decreasing). For those enduring SSRIs withdrawals, the privilege of being able to weather acute attacks of the zaps & sweats in the foetal position in your own bed and not a toilet cubicle at the office, was a blessing. WFH enabled many a third or fourth attempt at tapering off to be the final one.
This growing demographic have either managed the tapering off with zero pharmacological assistance or they have done so with one or a combination of any of the dozens of promising treatments for the above conditions from cannabinoids to psilocybin to MDMA (and anything else likely to be approved by the TGA/FDA in the coming decade).
So there’s an emerging number of people with THC going into in their system (as prescribed) at some point in any given 24-hour period, in almost every workplace in the country right now.
THC prescribed outside of working hours with reasonable reliance to be had on communications from the prescriber as to a minimum 12 hours between onset of impairment and sitting down at their desk the next morning.
A worker disclosing their being prescribed a minimal dose of THC, where the the therapeutic intent is that the effects of CBD are more pronounced when a dash of THC is added (ie someone prescribed a 3:150:50 THC:CBD:CBG and zero prospect of them being even remotely impaired).
Cases dealing with management of physical pain where a very low dose of THC is clinically defensible and no cognitive effects are likely to be discernible.
Cases where a request for use of THC during work hours, on work premises, would on any view of the full facts, be unreasonable.
WFH and daytime dosage prescriptions for THC that, as a result of traditional cannabis stereotypes, causes an employer to raise a concern at the cognitive ability of a worker to perform their obligations and produce deliverables within the timeframe required.
How to maintain consistency with consumption of alcohol policies / other prescription drugs?
How to ensure safe workplaces for everyone? Not just Joan for HR or other examples provided, but the people who have to work with them. In Slough UK or Scranton PA, we need a sensible approach to what is essentially, a worker taking their prescribed medication as directed.
Employers want to head off Van and Munter’s life dream of ripping bongs at work. The tea break was arguably the earliest workplace right achieved in the Industrial Revolution. The owners of the means of production figured out that a caffeine and dopamine boost in the afternoon actually boosted overall productivity and reduced accidents. All that from a plant hey?
What parameters ought be set around environments where a sudden onset of a moderate to high dose of THC causes a person to become a WHS risk? What arguments in favour are there for such a scenario to be viewed separately from the sudden onset of large amounts of alcohol?
If Joan from HR is recovering from surgery or managing chronic pain and if Joan does nothing but sit at a desk and work, then the risk level is not the same as office drinks, on office premises. It is certainly possible to take a low dose of THC that treats pain whilst at the same time does not cognitively impair due to being balanced out by other cannabinoids, plus if Joan is a trooper, many years of tolerance. Maybe “the good biscuits with cream” start disappearing from the kitchen at a faster rate. That surely is about the worst of it for Joan.
We expect employer solicitors will seek to argue that it is an unjustifiable burden on an employer to have people at the risk of known/unknown impairment by way of THC on work premises during any WHS misadventure/event. What is the worst case scenario? Tony from Marketing sprinting back into a fire to rescue the Peanut M&Ms he put in the fridge that morning? Perhaps employers will argue that people who consume THC over time, even at low doses, believe themselves to be inflammable. We don’t really know and we won’t really know until such outlier cases happen, if indeed, they ever do.
If Joan from HR isn’t impaired by THC then it doesn’t require an extra fire warden to carefully shepherd her down the fire escape even if Joan can’t be designated as one herself.
However if Joan was WFH and needed to bump up her THC dose a bit higher to manage a flare up and was then physically impaired but capable of working at a keyboard and doing her job, are there any WHS angles that restrict her from doing that?
These are things we need to figure out so we thank Messrs Kingston Reid for extending the conversation.
As MC makes further in-roads, employers will, on-the-whole, gradually become more accommodating to it or else it will cost them good employees. It already is. An employer’s level of tolerance to MC will no doubt be connected with any associations (positive or negative) with productivity first and safety second, because that’s how our current economic system rolls.
Operating vehicles on public roads?
Let’s start with the one point in this article that we all agree on. Mr Stutley is sort of correct when he says that from a WHS (work health and safety) perspective, where the job role requires driving on public roads or having a clean license then any workplace lawyer looking to argue reasonable accommodations for a worker on prescribed THC is going to be hamstrung by drug driving laws generally IF driving is part of the job or IS the job. This is why Drive Change is branching out into the workplace sphere. There are collaborative solutions to be had by continuing the workplace and MC conversation.
There are serving police officers in WA, prescribed MC for PTSD who have been accommodated on reasonable adjustments for five years now. They don’t punt them from the force. They just don’t let them drive or do any actual policing whatsoever and restrict them to administrative desk duties. It’s not an ideal life for someone recovering from PTSD caused from being a front line worker but at-least the mortgage keeps getting paid.
Where “not driving” can be accommodated without an employer incurring a loss, then it ought be a reasonable adjustment in the best interests of retaining a valued employee.
Employers can’t tell the diff btw prescribed and illicit THC?
If the worker has a prescription from a doctor stating the workers is prescribed THC then that is the only thing that matters re identifying the source of the THC.
Would any employer, anywhere in Australia, dare question the providence of opioid metabolites in an employee’s urine where that employee produced medical evidence indicating the drugs were prescribed? No. Cannabinoids ought be afforded the same “presumption of safe prescribed use.”
THC impairment is a cumulative concern that increases over time depending on the length and use of THC?
We would be happy to see the studies that KR base this opinion on. We know of one massive resources employer that recently instituted a policy on prescribed THC that relied on this ground also (cumulative use). The argument is that over time, persons who consume THC on a daily/nightly basis become an impairment risk 24/7. This, to the best of our knowledge, is predicated on studies done in the mid 1970’s where chimps and other animal subjects were forced to smoke 70 joints a day. BUT, we’d be keen to see whatever studies Mr Stutley has viewed and adjust our views accordingly. It is not at all unsurprising that studies which made the subjects consume stupidly high-THC cannabis reported adverse outcomes for the trial participants.
The overwhelming majority of medicinal cannabis patients are being prescribed cannabinoid ratios with nowhere near enough THC to replicate the exceedingly high doses of THC that the earlier cannabinoid research is predicated upon. Prohibition era scientists did a lot of work that doesn’t stand up to scrutiny against the measurable harm reduction results being achieved by doctors and other medical practitioners working in The Australian System of scheduled cannabinoids as medicines available via prescription.
Right now, let’s take the hill in front of us. We at Drive Change are specifically looking for cases where medicinal cannabis patients are only consuming THC at night with the minimum 12-hour break (and solid sleep) before fronting up to work the next day (invariably fresher after a sleep on CBD:THC and without day-after benzo/sero/z-class fog).
No-one, right now, would have buckleys of reasonable accommodations being made so they can consume an impairing dose (whatever that may be for that person) of THC on the job. Obviously for any manual job involving heavy machinery or heavy things moving on tracks at speed, this will always be out of the question. Whatever your prescription says, it is unconscionable to get high/medicated on THC when you’re working around other people in high risk environments. All it will take is one idiot to do this and other workers to die or be seriously injured and the cause of “Not Having to take SSRIs for the Rest of My Life” (with all the emerging risks that entails) will be set back years. That’s a cause example picked at random. There are hundreds of them that find their way to Drive Change the right to drive and the right to work so often comes down to one really shit choice:
“Do I have to keep taking [X Inneffective and/or Dangerous Prescription Medicine] for the rest of my life in order to be able to hold down my source of income?”
A Melbourne Storm Fan named Will Williams.
The discussion on reasonable adjustments and what is/is not an unjustifiable hardship needs to be had.
For the clerical and administrative and legal classes (office workers), meds that prevent you from operating heavy machinery ought be none of the bosses business when you solely punch a keyboard and click a mouse all day. There are 1001 ways to get out of fire warden duty so this risk is minimised for all parties concerned. One should always seek independent legal advice on these things and this article is most certainly not independent legal advice. Every worksite/office has an overlay of land law/lease restrictions and varied obligations to who can/cannot be on the premises.
The Fire Warden Argument?
This is literally the only THC and WHS issue that we can think of re white collar work/standard office environments. Perhaps Gerald from Accounts could be a risk if he puffed on a THC cartridge break on smoko, then accidentally spilt boiling hot coffee on Joan from HR. This West Aus piece frames it as being the sort of scenario that would require an employer to make unreasonable accommodations for a worker on prescribed THC by NOT making them the fire warden or a first aid officer. Let’s perhaps explore the class of persons ordinarily excluded from being fire wardens or first aiders (or temporarily excluded from acting in those capacities due to a temporary impairment). Let’s look at what sort of accommodations get made there and weigh up how much of a costs imposition they are.
The THC and WHS risks for office environments are, from a workplace insurer’s perspective, likely to be treated same as alcohol. Firstly, in standard office environments, it is no more an employer’s business as to whether an employee has been prescribed an opioid or a cannabinoid. Secondly, the West Aus argument that medicinal cannabis creates an unjustifiable hardship on employers who need to rotate people on/off a First Aiders/Fire Warden roster is certainly headline grabbing.
Vape cartridges on the sly combined with office drinks might get messy though. It might also result in people consuming much less alcohol and less boozy work culture all around. Who knows, this may result in greater productivity.
What are the issues with WHS insurers and office environments?
At the heart of it is the scenario where a white collar employer, by their conduct, acknowledges that a worker is on prescribed THC whilst at the same time knowing they have no sure-fire way to determine impairment should it ever become an issue should “shit happen.”
IF there is a WHS issue, then this is going to be a risk. However, it’s not the inflated risk that West Aus makes it out to be in standard office environments. The fire warden thing is an outlier scenario.
Two neuropsychiatrists and an interdisciplinary team to determine THC impairment?
Again, would be keen to see whatever literature they base this one on but it honestly wouldn’t be surprising if a bunch of psychopharmacology-neuropsych boffins validated their own existence by creating a set of standards and procedures and published them with the barest skid mark of peer review.
Irresponsible people who are stupidly high on THC during working hours will always get caught out by everyman detection methods. Smell, eyes and behaviour. How those initial conversations go are key for any worker should “shit happen.”
Although roadside swabs have their own faults, we here at Drive Change have heard of employers within the medicinal cannabis industry going to the extra expense of acquiring high-end oral swab tests that can reliably detect THC consumed within the last 72 hours and combining those swabs with various forms of manual impairment testing. That is some progress at-least.
It really isn’t an unreasonable expectation for employers to expect employees prescribed THC products to not consume them and come to work high.
An inferential leap of confidence to read this into a one-liner medical certificate?
Here is where we also partly agree with Mr Stutley. One liners or bare minimum letters stating the product names and dosages are not helpful. This is why the first step after a failed workplace drug test is to get the worker into an MC prescriber that has F2F capacity for the purposes of obtaining the sort of letter that lessens the length of the inferential leap that an employer is asked to take.
Is it too much to ask in 2023 for employers to trust their employees will only consume their meds in accordance with the detailed instructions provided in a properly set out doctor’s letter? This has been the standard course of action for opioids, benzos, gabapentinoids etc. No one cares about SSRIs because so many people are on/off them at one point in time or another that society would collapse if everyone had to come off them. With the exception of acute withdrawal phases, it’s fair to presume that they are not ordinarily deemed impairing (even if you lock your keys in the car a dozen times in three weeks and regularly lose things). SSRIs make people forgetful and foggy. To the extent they become a WHS risk? Perhaps one day we will find out.
Medical certificates involving a tick n flick done over the phone or online? Fair to query what kind of employer would accept that at face value without something else to provide a more fleshed out expectation about what the overall WHS risk would be. Products, dosage, timing. Product names like Super-Wizz-Bang-Cherry-Sherbert-Rainbow Kush do not help the cause of corporate-industrial integration of cannabinoid therapeutics also.
However it’s grossly unfair to question the origins of the THC in a positive workplace drug test where a prescription is provided.
Last week, the Road Transport Amendment (Medicinal Cannabis – Exemptions from Offences) Bill 2021, was voted down by the Liberal-National and Labor parties.
Those in favour of drug driving law reform were defeated in a 29-6 vote.
Prior to last night’s debate, Drive Change wrote to all Members of the Law and Justice Committee, highlighting that medicinal cannabis remains as the only prescribed medicine that does not have a legal defence for driving.
At the end of the vote, a snide comment was passed by one of the Members (the Hon. Mark Latham MLC) to “pass the bong,” with the Road Ministers laughing at this remark. This childish antic is one in a string of out-of-line
Such appalling behaviour should be called out. There have been over 250,000 approvals for medicinal cannabis in Australia, and this sort of language is disrespectful to the thousands of patients with lawful approvals. Australians who have been approved for medicinal cannabis, but particularly to patients who have had their license taken away, lost their job, their livelihood, and quality of life due to these drug driving laws.
In reducing the stigma around (medicinal) cannabis, it is important that we curb the use of insensitive language.
Such language and remarks from Mark Latham highlights the stigma, discrimination and criminalisation around this medicine.
In order to change this, we need to remember to make sure Australians who are treated with medicinal cannabis are spoken of respectfully. There needs to be a shift in our perceptions, a change in how we speak, and most importantly, we need the laws to change. With the most recent Parliamentary defeat, the law remains discriminatory against these patients.
You can view the debate below:
Share your story and write a letter to the Chair of the Law and Justice Standing Committee (the Hon. Christopher Rath) office.rath@parliament.nsw.gov.au
The goal of Drive Change is and always has been about advocating for new driving laws where medicinal cannabis patients and doctors get fairly treated. To achieve this goal, we’re doing all that we can to have the discriminatory drug driving laws changed to protect all those legally opting for medicinal cannabis. Without our ambassadors and donors, we wouldn’t be able to do this.
You can read more about the backwards science of the laws here.
We believe it’s important for our current and future ambassadors and donors to know how their money is put to work. Here is a round-up of everything Drive Change did to push for drug driving law reform in the past year:
Nationwide Petition
We worked with doctors, scientists, and medicinal cannabis patients to gather the information we needed to present a petition asking the community to show their favour for drug driving law reform. The goal, this petition, is a vital tool in the fight.
The petition remains live with over 24,000 signatures. You can sign it now or share the link and help us reach 25,000 (and beyond).
Showing Parliament the people in support of medicinal cannabis reform, by the numbers, helps strengthen our cause to have change enacted.
Ask Me Anything
Hosted by industry experts, this event invited the public to virtually attend a panel where they could pose any question they had regarding drug driving laws and medicinal cannabis. We were honoured to have a panel of experts including Dr Teresa Towpik, Dr Thomas Arkell, former police chief Mick Palmer, and MP Fiona Patten.
Events like this are important to connecting patients and doctors in the community with leaders in the industry who can be teachers and advocates for the medicinal cannabis industry as a whole.
This closed-forum meeting welcomed government and industry leaders to discuss the current laws regarding science, industry, and overall health and safety of our roads and community members. In doing so, we are creating time and space for law reform to be a serious discussion amongst those who have the power to create the change.
Our network of supporters and ambassadors include several of these industry leaders and members of Parliament. If you are interested in joining them on our team of ambassadors, please email hello@drivechangemc.org.au for details.
‘Letters to Local Members’ campaign
Drive Change believes that getting the voice of the community heard is integral to the process of drug driving law reform. That’s why we organised the ‘Letters to Local Members’ campaign.
Through this work, we made it easy for the community to send letters to their local members urging them to consider amending drug driving laws to protect medicinal cannabis patients.
It also served as a way for the community to urge their local representatives to join the Government Roundtable and become part of the discussion.
Getting in touch with your local representative is one of the best ways to fight for change. You can still write a letter sharing with them your own reason for wanting change. Find out how: Write a Letter to My Local Member
Submissions to Parliament
Shortly after writing letters to local members, Drive Change set up community members with the chance to lodge a submission in support of the NSW Road Transport Amendment Bill.
Introduced by Cate Faerhmann and up for debate this year, community support for this bill is integral to pushing for change. As with every other opportunity to see drug driving law reform, Drive Change worked diligently to make sure the community’s voice was heard in this matter and all others.
Nimbin/Mardi Grass Drug Driving Symposium
Rounding out all of our efforts this year, Drive Change leader and former Magistrate David Heilpern appeared at the Australian Medicinal Cannabis Symposium. He spoke about the discriminatory drug driving laws and how they are harming patients, public health, and economic growth.
What’s Next?
Support from the industry and community is essential to the continuation of our work at Drive Change.
For industry leaders and product suppliers: Support patients and doctors who rely on you to access medicinal cannabis. Email us at hello@drivechangemc.org.au to find out how to become an ambassador.
For community members: every little bit from you helps us fight for fair and equal drug driving laws. We thank you for your support.
Lawyer Mat Henderson shares his reflections on possible ways around the drug driving law impasse and his experience defending a professional driver (and die-hard Storm fan) who was penalised for medicinal cannabis.
“It’s the attainment of justice and fairness that gives lawyers their buzz.”
So said The Hon Michael Kirby during one of the dozen visits to UTS Law School during the 00’s. The truth is, there is little to no buzz for a lawyer doing pro-bono work for medicinal cannabis cases. After five years of this sort of work, I can attest to that. What it really is is a grind of hearing heartbreaking patient stories and organising of doctors’ letters, which all feels more like shoveling sand against the tide than it does practicing law.
The lack of buzz stems from an inability to “change the law” in the time-honoured way by approaching courts, arguing the distinguishing facts of your case, setting a precedent, and changing the law (a gross over-simplification).
It doesn’t matter if “Granny Scroggins” is a cancer patient who last consumed her prescribed THC a month ago but then stopped being able to afford it. If it is detected in a roadside oral fluid drug test, she’s breaking the law. These laws seems to suggest that presence is presence and criminality is criminality. Even if you never thought of yourself as a criminal, as Granny Scroggins never did. If THC is detected in your system, you are.
In every Australian jurisdiction (bar Tasmania), it remains illegal to operate a motor vehicle with any detectable level of THC in your oral fluids.
Don’t even sit in the driver’s seat of stationary car if you had your THC-containing medicine today. It’s a zero tolerance approach to any presence of THC. This law persists, despite the increasing number of international jurisdictions which are adopting a per se approach, i.e picking a measurement of THC-in-blood and only making it a criminal offence to drive if that level is detected.
Whether it’s Granny Scroggins or your cousin Cody, the unjust drug driving laws can have serious consequences for medicinal cannabis patients.
The basis of our road laws are inherently flawed
A zero tolerance approach focused on saliva testing is fraught with accuracy issues. The current police practices take your saliva sample and sends it off to a lab. There, it winds up in a whizz-bang machine that looks for evidence of THC in your fluid, regardless of how long ago it was consumed. THC consumed days or even months ago can show up through this method. Whether it reads a faint positive or false positive, the law doesn’t care. What this machine spits out is essentially the live or die results of your driving priveleges.
Australians don’t want unruly and impaired recreational consumers of THC on our roads.
Nor do we want people impaired by their lawful THC meds to get behind the wheel when they bloody well should not.
These are a given.
Australians also trust each other to be responsible when it comes to taking any prescribed impairing medicine (as directed) and to not operate cars, mix the medicine with booze or use heavy machinery if they feel impaired.
Common sense dictates that most folk apply the ‘next day rule’ to impairing drugs. This should also be a given when it comes to medicinal cannabis but law makers appear to be blocked by law enforcers. This is not how the separation of powers is meant to work.
How Parliament is Working to Change the Law
If you got this far, you may or may not know about the Parliamentary developments in Victoria and NSW.
For those who need to be caught up, the decision was: “More research required.”
Over the last ninety years, police have professed to be experts in determining whether or not a person is affected by cannabis/THC. Now we’re essentially told that such rudimentary policing skills are beyond them and that whiz-bang machines are more reliable.
Righto then. Below is my personal account of what will likely continue to happen whilst the research progresses.
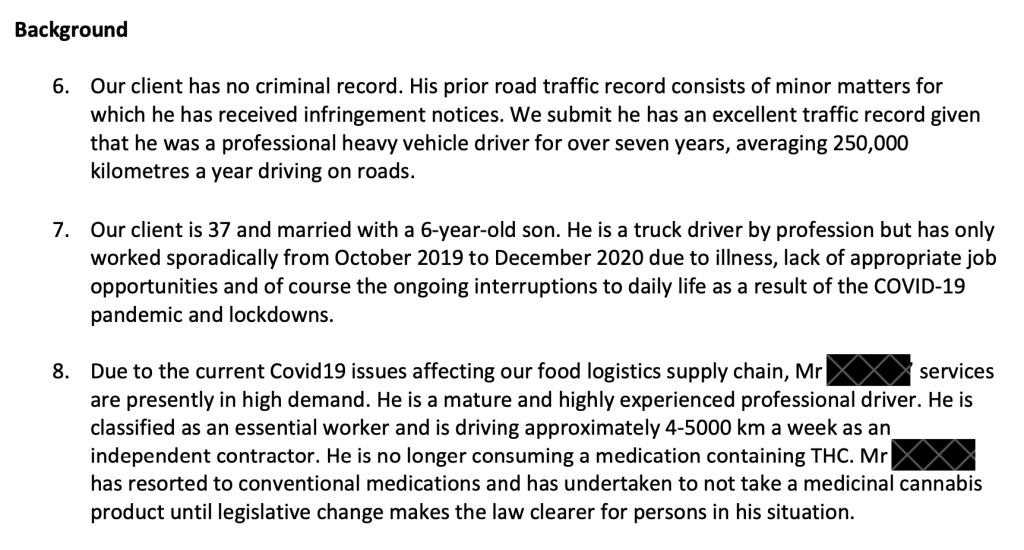
Mat Henderson’s Tricky Tale of Defending a Medicinal Cannabis Patient
Two years ago, I took a call from a friend who works in the locally-licensed medicinal cannabis space.
A doctor had just called them about a patient on a 50:50 product who consumed 0.25 of a ml of oil (approx. 2.5mg CBD and THC) at 8am and then got pinged by a roadside drug test at 4pm. The patient is a professional driver with a bad spinal injury and felt no adverse impairment that day at any time during the day of offending.
“His name is Will, “he’s a Storm fan and he’ll make sure you’re aware of it.”
More about Will later though. First Let me firstly give you a flavour of the factors you need to weigh up when working with a person about their history of prescribed THC, traffic history, and logistics around the day of offending.
Any reasonable person would be able to understand there was no impairment from medication on Will’s part. But that doesn’t matter; what matters is how the law is written.
The way the laws are currently written, unless you have a reasonable explanation for how the THC got into your saliva passively (and possibly without your knowledge), a court is in no position to do anything other than apply the law and mark your actions as criminal.
Detection of any amount of THC results in the minimum penalty 3-6 months loss of license.
If you’re given a fine and purport to contest it on any grounds other than passive/unknowing ingestion of THC, you’ll find yourself in a legal cul-de-sac without a defence that a court is able to spend any time listening to. Best you don’t go speculating on how reasonable your reasonable explanation is without seeking formal legal advice. This blog post is not that.*
When I do offer legal counsel to clients, I commonly hear the same story:
“I am a lawful medicinal cannabis patient”
“I take my medicine lawfully.”
“I’m not some scallywag kid driving when stoned.”
Sadly, none of these remarks are a good defence as the law remains as it is. Having detectable levels of THC in your saliva is a punishable offense, and patients ought to think twice about blurting out this knowledge after returning a positive roadside THC test.
If you know how the THC got there (and it was from consumption of your prescribed medicine), please don’t expect the police to use that information to apply leniency and wave you on.
However, if you’ve thoroughly educated yourself on the futility of arguing a medicinal defence and understand that if you contest the fine, you’ll inevitably end up pleading guilty, then you may wish to seek leniency in sentencing. If so, keeping your story consistent in any dealings with the police and the courts is always wise.
Always consult your doctor if you return a roadside THC positive.
Ask nicely and your doctor should write a supportive letter to the court outlining what conditions you’re diagnosed with, what medications you’re on and their brief opinion as to the efficacy of those medicines and any overall symptom relief and improvement in your quality of life.**
With such harsh and unjust laws, what could any leniency look like?
Well, perhaps you may not have conviction recorded or face an unsettlingly large fine.
Like I mentioned at the start, there’s no justice buzz for lawyers here. Not when every THC detection matter feels like nailing jelly to the ceiling, fighting a retreat with the British at Dunkirk or fighting against them at Ruapekapeka, massively outgunned but most certainly not out-witted. On most facts, a scrappy draw is the best result you can ask for.
The preservation of a future career working on the Canadian ski fields is a lifeline for some people. A criminal conviction in Australia tips poutine all over plans like that. However, if a person has to revert to previous medications like opioids and benzodiazepines which may well kill them in order to avoid offending in the future, then it’s hard to interpret that as anything other than a loss.
Losing all the time sucks.
It’s rough terrain for medicinal cannabis patients and lawyers looking for a win against the current drug driving laws.
Despite knowing this, I still wanted to speak to Will…
This was back during the first lockdowns of the pandemic and there was a strong public interest in ensuring food supply networks remained functional. Lawyers chasing the fairness buzz, like good reporters, are always looking for good facts. Surely such facts warranted a letter being sent to the prosecution to seek withdrawal of charges that Will was facing on public interest grounds.
Either way, after a long chat with Will, it was clear he had a unique factual matrix worth exploring and even if there was no joy to ultimately be had in court, there was the prospect that the case may have communal learnings for all in the drug law reform space.
Coincidentally, it was also around this time that Drive Change was founded, and David Heilpern was roped in to consult pro-bono. Greg Barns SC was instructed to appear and graciously agreed to do so pro-bono as well.
This is where things start getting lawyer-ly
Everything about Will’s circumstances warranted a request for some prosecutorial discretion. Through endless lockdowns, delays, illnesses, and adjournments, this approach was initially taken twice. First with the police prosecutors at the Magistrate’s Court. They stated the prosecution would proceed. Secondly with the top Victorian prosecutor at the Office of Public Prosecution where, in April of this year, they also stated that the prosecution would proceed.
Excerpts from those reps drafted by me and settled with David and Greg below.
On 11 August, Greg appeared for Will at Heidelberg Magistrate’s Court. In the absence of a defence as to how the THC got into his system, Will pleaded guilty.
In being deferential to the presiding judicial officer, we shan’t regurgitate their words verbatim, less to say that the court was moved by Will’s supporting letter from his doctor and his attempts to have a more functional life beyond opioids. There was no fine payable and no conviction recorded but the court was compelled by law to suspend Will from driving for 6 months. Will was given the lowest possible penalty just as Greg wrote submission that Will is “ultimately a victim of the Victorian legislature’s failure to keep abreast of the development of medicinal cannabis as a legitimate form of pain relief.”
Will has had some time to plan around the inevitability of a license suspension but still, it’s hard. He tells me a McDonald’s has opened in walking distance from his new place. He can bang out some hours there to keep some funds coming in.
He shouldn’t have to work at Maccas for 6 months because of being a lawful medicinal cannabis patient who drove whilst unimpaired. Yet with detectable levels of THC in his saliva, that’s what he’s faced with. All medicinal cannabis users ought to be afforded the right to drive provided they aren’t impaired by THC (to Maccas even).
The best approach to testing for THC
Due to the vagaries of THC and human metabolism, it’s not looking mega-likely that sampling your saliva or blood and reverse calculating the timeframe in which you *may have* last consumed THC is going to be possible anytime soon.
Sure, there’s cannabis breathalysers in the R&D pipeline but thus far they are capable of detecting smoked and vaporised cannabis, not orally or sublingually ingested THC.
Suppositories? Forget about it. Even if there was a device on the market that purported to test for ingestion of cannabis via anal suppository, I imagine that both the police unions and civil libertarians would unite to oppose its use.
Basically it seems as if The Man is unwilling to budge on the issue of THC detection until such time as someone in a white coat provides them with the equivalent of “0.05 on the Willie Nelson Dial” (as they see it) and the means to conduct the test within in a roadside mouth-swab oriented environment.
The law, in my humble opinion, as it stands in this area, is an ass.
We have a set of laws on our statute books that unfairly target a growing swathe of the population with the unnecessary stain of criminality. This is an unsatisfactory state of affairs. Given the outcomes of the recent Parliamentary reviews referred to above, it is a status quo that will continue for however long it takes for the research to be done, then peer reviewed and published.
Q. How long will that take?
A. Probably five years and as Bowie sang in Five Years, my brain hurts a lot.
I wish this article contained a happier call-to-action beyond sit down, shut up and wait for the scientists to finish whatever it is they do behind their velvet curtain.
Where to from here?
When the callout comes for trial participants, best we spread the word far and wide. How about a temporary statutory defence (for THC detection) being afforded to participants registered in the studies recommended and supported by the Victorian parliamentary review and similar studies (seemingly) endorsed by the NSW review and soon to be debated on the floor of Parliament?
The more people who don’t have to put their regular lives on hold in order to wind back the mysteries and wonder of cannabinoid science, the faster the damn research is going to get done.
The biggest hidden hold up to the research is securing clinical trial participants for a THC and driving study. A study which would prevent them from driving whilst the research is being carried out. If parliamentarians allow absurdities like this to stand then our grandchildren are on track to living in an idiocracy where sugary electrolyte drinks are what plants crave.
Instead of being quiet and patiently waiting for Bunsen and Beaker to turn in their paper, we in NSW and Victoria can ensure our votes go to candidates with some chance of setting up a balance of power in upcoming state elections. The Queensland government are about to announce a parliamentary review into drug driving laws and medicinal cannabis. Maybe that review will involve some genuine consideration of the practicalities involved with implementing an interim regime based on best practices from Norway, New Zealand, Canada and Ireland. Perhaps the per se limit of 3ug/L THC in blood as is used in the Netherlands could be a good starting point. If you consumed THC within the last 15 hours, you’ll likely get pinged.
Any researchers who wish to assail me on the accuracy of that, please provide your own estimates of when the average male and female who are daily consumers of, say 20mg of THC would ordinarily be safe to drive after their last puff on the Mighty Medic. The Dutch have gone with 15 hours, based on what we know of vaporised ingestion of THC, is there any chance of bringing that non-drive time down under 10 hours? 4-6 even?
Internationally, blood draws are common.
The logistics for increased use of blood draws in Australia are many, complex but not insurmountable. Anyone suspected of impaired driving can be sent off for bloods under current laws. It’s just that if we sent every person who returned a THC positive in saliva off for a blood draw – it would cost lots of money that governments don’t wish to spend and involve police time that the police would prefer to invest elsewhere.
Any relief against the current zero tolerance regime will be welcome, even if that is by way of a very broad legal limit of THC in blood that doesn’t yet have a strong correlation to being unsafe to drive, yet serves the purpose of deterring people from consuming THC and driving within timeframes where they may be impaired. Hopefully, researchers can narrow that window down further from 15 hours but until they do, perhaps this is where the compromise lies.
Until such an interim compromise is reached, outcomes for people like Will only serve to undermine the rule of law.
What do those words actually mean?
It’s problematic for faith in our courts if growing numbers of people feel that the rule of law is not there to protect them but is seemingly out to harm them by removing their right to drive a vehicle and participate in as functional a life as possible. The more people who feel that way, the more that the laws are ignored and violated to the point where they’re still “good law” but they are becoming increasingly ineffective as laws-to-be-obeyed because knee-jerk adherence to the rule of law is undermined by the unjustness of it all.
When punishment that is solely punitive (and not at all remedial) is handed down by courts to people that the overwhelming majority of the population don’t deem to have acted like criminals – that’s when you can say the rule of law has been undermined. When judicial officers step down (thank you David) rather than continue to apply such laws, that’s the alert signal that the undermining is happening right now.
Please continue to forward your hard luck medicinal cannabis and driving matters onto me. The facts will come and the law must change.
—
Mat Henderson is the principal lawyer of Reparation Legaland legal lead for Drive Change. Writing on Gadigal Lands and Waters. Always was, always will be. Ka nui te mihi ki a koutou.
*Although ostensibly an article about THC and drug driving law reform, nothing herein is intended to be construed as legal advice. Everyone’s circumstances are unique to them and unique to the idiosyncratic processes by law enforcement in every state/territory. If you need that advice, then by all means contact me.
Don’t print this off and wave it in front of a police officer’s face as if it’s the Magna Carta because it isn’t.
**If your medicinal cannabis prescriber does not wish to provide a letter to the court or if they wish to charge you for the privilege, then also please contact me. If your doctor is seeking guidance on how to write such a letter, have them get in touch with Drive Change.
As medicinal cannabis becomes a more popular solution for patients and prescribers, it also becomes a bigger source of economic growth. Last month, industry leaders gathered together at the Australian Medicinal Cannabis Symposium to discuss triumphs and roadblocks of the budding medicinal cannabis industry. Drive Change lead and former magistrate David Heilpern was there to share his insight on how discriminatory drug driving laws are harming patients, public health, and economic growth.
“This is an industry that’s starting to attract big business from funders who obviously see it as financially viable,” said David Heilpern, referencing medicinal cannabis investors, “I think they’re kidding themselves while these drug-driving laws are there.”
Of course, it’s not just the industry that these drug-driving laws harm, but individual patients and entire communities. Most patients who deal with pain rely on driving to work or just living their daily lives. Though medicinal cannabis remains an illegal substance in the eyes of road police, other impairing pharmaceutical drugs–and drivers who take them–are well within their right to drive while using their medication. These alternatives include benzodiazepines or opioids, both proven through extensive scientific studies to have a greater impairing effect on drivers than cannabis.
David Heilpern is a staunch advocate for fair and equal drug driving laws.
“If it was about road safety, it would apply to other prescription drugs,” Heilpern said of the current drug-driving laws before asking rhetorically, “so who wins from this?”
The answer, of course, is clear. Pharmaceutical companies who make and distribute drugs like opiates, benzodiazepines, and other impairing drugs have monopolised the healthcare system for decades. For many years, these drugs were doctors’ and patients’ only options for combatting pain. We know better now.
“Most people using medicinal cannabis were using pharmaceutical drugs to start with. And they’ll go back to them, even though the evidence is that those drugs have a greater impact on their driving.”
David Heilpern
According to the TGA, clinical studies have proven that patients who are prescribed medicinal cannabis report up to a 50% reduction in pain (especially for neuropathic pain, arthritis, and fibromyalgia); improved sleep and quality of life; and improved anxiety symptoms. Medicinal cannabis has also shown efficacy in reducing symptoms of epilepsy and muscular sclerosis, and it can alleviate the side effects of chemotherapy for cancer patients (although this practice is not yet approved in Australia).
Many patients find better relief from their pain and discomfort when taking medicinal cannabis than traditional drugs, and enjoy a life free from the cumbersome side effects. Unfortunately, because of the law, they have no choice but to deny medicinal cannabis prescriptions.
“Patients go back to their opioids and they drive on the roads probably far more dangerous than they would have if they had taken that [medicinal cannabis] prescription,” he added.
Legislators continue to argue that medicinal cannabis is going to be a problem–but places where it is legal prove the opposite. We don’t even have to look far to see the effects of legal prescription cannabis in drivers. Tasmania legalised medicinal cannabis on the road in 2020.
They have seen no increase in road toll since.
How can we catch up on the mainland? Now that the tides have changed in government, we might have a chance to have our cause heard.
Now more than ever it’s important to write to your local member. Let them know how the drug driving laws affect you, your family, or your loved ones, and direct them to scientific research to back your claims.
You’ll find all the details you need on our BetterLetters campaign page. All you need to do is send the letter and start urging them for change.
If Tasmania can do it, so can the rest of Australia.