If your prescribed medicine prevents you from driving and working, what does that mean for your human rights?
The UK’s Cannabis Industry Council released a report this week into workplace issues for medicinal cannabis patients who are regarded as disabled under UK work, health and safety laws. Despite its specificity, it is a worthwhile read for us in the Australian space.
Similar issues are arising in Australian workplaces. Employers are mostly standing people down/moving them on or not hiring them at all if prescribed THC becomes a live issue.
When it comes to the British colonies of the Australian mainland and adjacent islands, Workplace laws ought be clarified to explain that when an employee asks for reasonable adjustments to be made on the basis of a temporary illness/permanent disability requiring them to take a medication outside of work hours that all medications ought be treated the same. As a Uno card, that’s a Draw Two right there. Problem being that employer medico-legal advisors flag unknown risks due to the current lack of an impairment proxy for THC. They need to cover their backsides and record that they advised their clients to exercise caution. The takeaway for many employers is “don’t hire the stoner, hire the other lady.” in work, health and safety terms, that’s a probable Draw Four.
Am sure that those who monitor the MC socials noted an uptick in hospo workers reporting pre-screener issues when a medicinal cannabis prescription is disclosed. These people are doing the right thing. As is usually the case when legal medicinal cannabis butts up against prohibitionist-era-oriented legal and social institutions, these people doing the right thing get punished for doing so.
How do we get this clarification that MC ought be treated the same as other prescription medicines? A few ways. With a series of sensible workarounds likely to be discussed in the upcoming Victorian LCA’s review/committee/process to have an adult discussion about fixing this so that the hospitality industry (at-least) doesn’t come to a screeching halt.
Another way is for clarification to be expedited by way of a matter/case with good facts and NO whiff of non-medicinal cannabis use going through various courts and tribunals. That will certainly provide guidance.
For readers who know him, it won’t come as a surprise that Veteran advocate Derek Pyrah is already aiming up at a Human Rights angle for all veterans to received subsidised MC, even on MH-only grounds. An opinion via a senior HR counsel is in the works but it will take some time. Derek’s arguments are also applicable to the MC and workplace and driving issues.
Ultimately it’s a question of whether Adequate Medical Care in Article 25 of UN Declaration of Human Rights means whatever The Literature says or whether there is scope for a human rights angle in circumstances where a person can demonstrate that harms were caused by an unwise and voluminous combination of prescription drugs over many years?
The DSM says that Derek received nine years of the best mental health care that any system could offer. Five of them separated from Missy as a result of being on psych wards. Everything from antidepressants, antipsychotics, sleeping pills and opioids. But all at once and in large amounts. You try lifting your head on 1800mg of quetiapine.
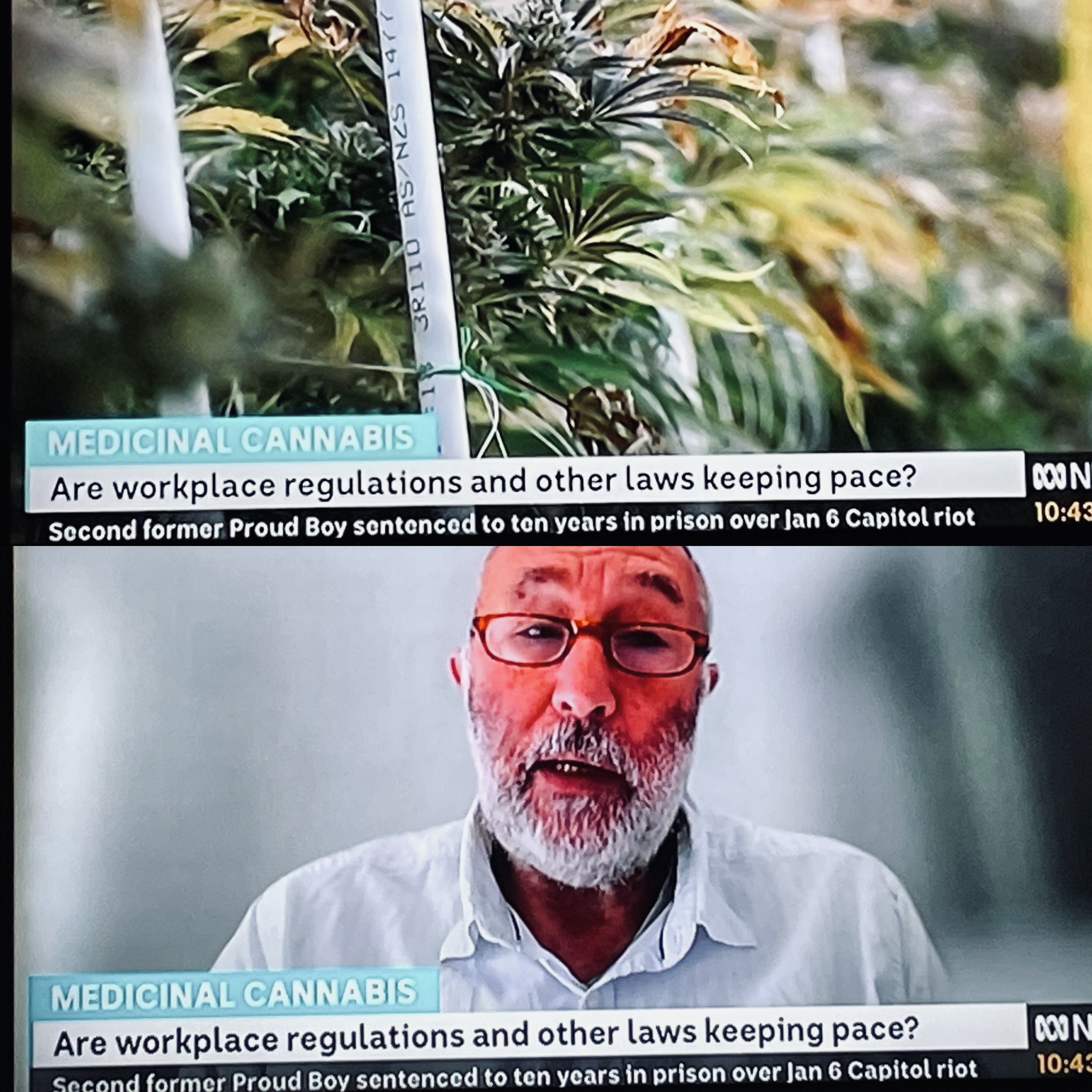
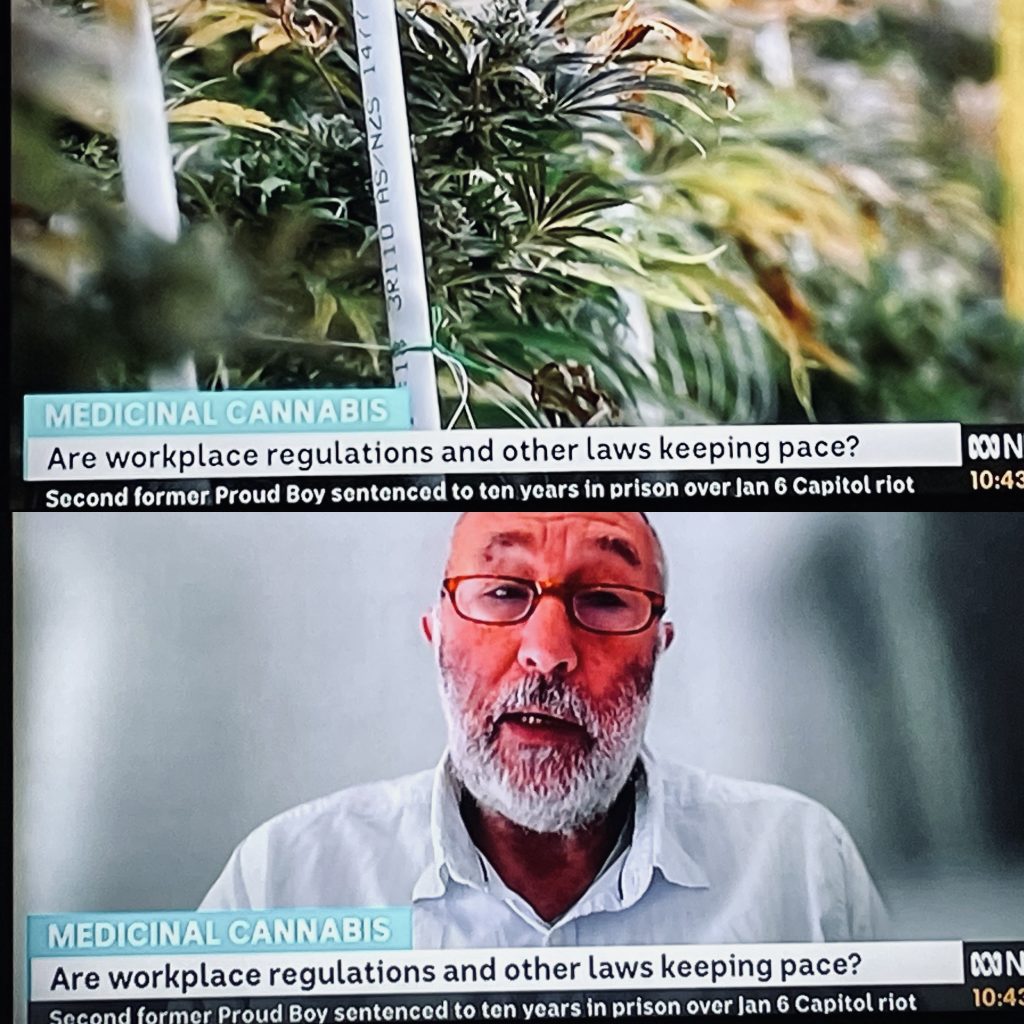
Is there a court on earth that would believe Derek’s subjective opinion on whether CBD:THC is more safe and effective for him than whatever the prevailing wisdom of the prestigious Medical Colleges and prevailing expert psychopharmacologists say? Would any of those academics accurately be able to tell you which picture of Derek below is the guy who vapes (but used to smoke) cannabis and which is the guy taking his many different prescription medicines as directed?

For workers faced with the conundrum of going back to the meds that didn’t work and/or harmed them, the immediate gut feel of adverse action being taken them is that their human rights are being violated. In some Australian jurisdictions this is worth a closer look when it comes to the nature of their work and the actions taken against them.
If a worker being prescribed THC oils or flos for nighttime/bedtime/non-work days only for:
- Specific indications “ABC/XYZ”; and
- As a harm reduction measure from many years of using tobacco spin and combustion + lowering overall THC consumption.
If you’re a doctor scratching your head wondering how you’re going to frame a letter to an employer for this class of patients then please get in touch.